Tips para el cuidado de su ojo
Lecturas ASCRS 2001
Nomograms
Publicaciones Del PDF
Estudio de casos
Touch and Go: A-Scan Technique
Kurt Buzard MD FACS
Tulane University Medical School
University of Nevada Medical School
Buzard Eye Institute
Las Vegas Nevada
A-scan Tips
- Hand held scans are inherently inaccurate
- Remember that accuracy to 0.5D requires about 150 micron A-scan accuracy
- This requires:
- precise positioning
- minimal or no pressure on cornea
- a wet cornea
- good spikes
A-scan Room

Storz A-scan Attached to Slitlamp
 |
|
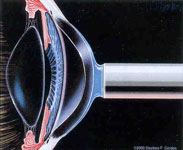
Touch and Go Method
 |
|
General rules
- The two eyes should usually match in terms of a-scans
- Assymmetrical refractions may reflect assymetrical a-scans
- For sulcus placement subtract 1 diopter
- For piggyback IOL add 1 diopter
- Aim for -1.5 to -1.75 D for monovision
A-scan Spikes
 |
|
IOL Calculation
 |
|
Keratometry
- Best measurement is manual
- Next best is Humphrey autokeratometer (not made anymore)
- Never use topographic k-readings
- Combined autorefractors/keratometers are just average for k-readings
Surgical Issues
- We do surgery 1 day to 1 week apart ... Think of patient in refractive terms, try ctl and possible monovision on other eye
- Better surgery results in more predictable results...faster surgery with complications can add many unnecessary postop visits and slow visual recovery
- Use astigmatically neutral surgery
After Surgery
- Three main issues:
- Capsular opacification
- Astigmatism
- Spherical error
- We see at 1D, 2W and 1-2M
- Do astigmatism at slitlamp..ATR sooner / WTR later since it may degrade
- Do IOL exchange for spherical error
Summary
- Refractive phaco is a state of mind
- Losing on a few cases with reoperations will be repaid with many other happy patients without reops
- Think refractive! ... Early relaxing incisions...astigmatically neutral incisions...and ctl for spherical errors will increase satisfaction and decrease visits
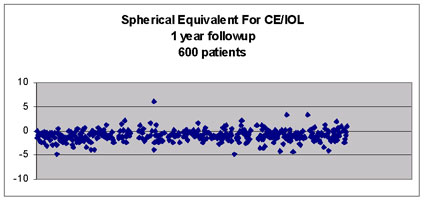
Refractive Phaco Spherical Equivalent for CE/IOL
Six hundred patients, 1 year follow-up