Blepharitis

What is blepharitis?
Blepharitis is a common and persistent inflammation of the eyelids. Symptoms include irritation, itching and occasionally, a red eye. In addition, blepharitis can cause the eyes to be tired and this condition can exacerbate dry eyes and allergies.
This condition frequently occurs in people who have oily skin, dandruff, or dry eyes. Blepharitis can begin in early childhood although it is more commonly a problem that develops later in life.
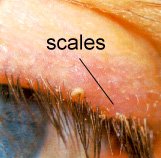
Bacteria reside on the surface of everyone’s skin, but in certain individuals they thrive in the skin at the base of the eyelashes or even enter the oil glands in the eyelid called meibomian glands. The resulting irritation, sometimes associated with overactivity of the nearby oil glands, causes dandruff-like scales and particles to form along the lashes and eyelid margins.
For some people the scales or bacteria associated with blepharitis produce only minor irritation and itching, but in others they may cause redness, stinging or burning. Some people may develop an allergy to the scales or to the bacteria which surround them. This can lead to a more serious complication, inflammation of the eye tissues, particularly the cornea. An important concept is the fact that blepharitis is a chronic condition, cleansing and any therapy needs to be continued for a long time (i.e. several months) to be effective.
How is blepharitis treated?
Blepharitis can be a stubborn problem. Although there is no specific cure, it can be controlled through a careful, regular program of hygiene. The problem is abnormal oily areas surrounding the lashes and plugged glands with abnormal secretions. The solution is the application of a warm washcloth for a minimum of 10″ over the lids to gently clean and liquify the abnormally thick secretions in the meibomian glands. After this a gentle scrubbing of the lids with the washcloth will squeeze the secretions from the glands.
If this regime is followed once or twice per day, over a 2-3 month period, the condition will gradually improve. The use of a clensing agent such as baby shampoo is not harmful but often causes irritation and in general is unnecessary.
Will medication help?
Many medications are available for the treatment of blepharitis, including antibiotics and steroid (cortisone) preparations in drop or ointment form. While cortisone medications often hasten relief of symptoms, long-term use can cause some harmful side effects.
Once the acute phase of the condition is overcome – a process which may take several weeks – milder medications, if any, may be helpful to control your blepharitis. However, medications alone are not sufficient; the daily cleansing routine described above is essential.
learning series let me just
our speaker for today today we have
an optometrist he finished his
bachelor’s at lotus college of optometry
and currently he is a phd candidate at
the university of alabama
his special interests are in myopia
optics and anterior segment and today
his ideas and his views on the treatment
blepharitis so welcome ku and
thank you very much for taking out this
hi um greetings everyone i know
we are at different time zones um sunday
morning for me sunday evening and night
but thank you so much for uh joining
and um i would like to thank
the ols series um especially for this
um and uh mr barodawala for
allowing me to present this topic and
share this information with you all
um without further ado i think i will go
okay so we are going to be talking about
treating demodex clepharitis
into that a little bit of my background
especially in this topic so i’ve been
working on a systematic review
um about treating demodex blepharitis
almost most of the past 18 months the
initially proposed uh almost two years
ago and then six months later
um it fell into my laps and i have been
on getting some information on this and
creating a comprehensive guideline sort
so i think uh that way i have learned a
um of this topic and i would go ahead
sharing the information with you all so
what we’re going to be talking about
is first what is demodex blepharitis uh
which i guess one of the audience member
um if i could share something about
demodex blepharitis so yes that will be
um and this is going to be very clinical
um it’s good i’m going to speak about
the diagnosis like how one can go about
in a daily clinical practice diagnosing
and the management um management of this
so i think the most important thing or
take home from this whole presentation
today would be is to remember that
demodex mites are present nearly in 30
of patients with patients with
demodex infestations are generally
undiagnosed and untreated till date
um we will go into a lot of details as
this is happening and uh you know things
like how we can do better
as a clinical community of optometrists
uh to improve the diagnosis and the
treatment of this condition
and the objective is to really
understand how to diagnose this
and the clinical management of how to
and make sure that they get the most out
for your services um this
so my journey started as i said almost
where it fell into my lab um almost two
my mentor dr andrew parker was
approached by the cochrane
database and systems review to do a
systematic review on demodex blepharitis
a systematic review is basically looking
research and scientific data on a
particular topic out there
and then putting it together in one one
document one piece of information
so that it can be accessible for
individual clinicians researchers etc
and they don’t have to look for
all of these thousands of papers that
might be available on the same topic
after a meeting by my mentor and he was
like looks like we’ve been offered to do
review and i was like okay what’s the
it’s demodex blepharitis and i’m like
huh sounds interesting now then as an
optometrist i knew what blepharitis was
um and but i did not know what demodex
in my head i’m like wait i don’t
learning ever at all about this topic
and my mentor is like so do you think
in like leading this out like yeah sure
i got it and um of course i didn’t want
him to know that i did not know what the
and so immediately afterwards after the
demo text blepharitis and yeah a couple
and looks like it is a blepharitis
and i’m like okay so this exists out
uh probably i just was sleeping in class
taught it at lotus so i decided to go
back to the olden and faithful
kanski clinical ophthalmology and
look up the word demodex in the index
um in my copy there was no mention of
and i was like that is weird then i
looked through the blepharitis chapter
and i could not find anything at all
i was like i haven’t even seen a single
um like or diagnosed or heard of this
time as a clinician so i was like
why is cochrane wanting to do a review
for something that is so rare they
generally do reviews for topics which
significant amount of information that
people might get confused
when they try to look it up and so i
a revelation that this this condition
and um it was a journey for me
to actually witness the start of a new
excuse my um covet references
uh throughout the presentation but i
uh so yeah and um i looked up kanski it
wasn’t there so then i thought okay
um i looked up at the in the eighth
edition which is the most recent one
what i used when i was going through
optometry and surprisingly
um almost one third of the demodex
chronic blepharitis condition in kansuki
in the eighth edition has been revised
to add demodex i was like okay
if they’re changing one third of the
topics as common as blepharitis
this might definitely be something big
and i should look into and read up at
uh knowledge and so that’s how the whole
um so that everyone is on the same page
um i will start right from the basics
as to what is blepharitis even though i
have gone through this like a billion
times since it’s one of the first topics
anterior segment uh in optometry so
blepharitis is primarily the
and there are lots of lots and lots of
it can be irritated and itchy eyelids
you can look at it as someone someone
might say they have photophobia
burning sensation in the eye
etc etc like dry eyes and anything
in that realm can be a symptom
for blepharitis what we generally
see on the slit lamp is gender fly
on the lids and lashes and
as you can see in the picture over here
tiny dandruff like particles at the end
and there can be many causes for these
and i will not go into the details of
this is about demodex blepharitis and
um and primarily there are two chronic
types one is the anterior blepharitis
and posterior blepharitis also if you
or so the khan skin twenties um the
if you open it up uh that there are
these two major types of blepharitis
uh the eighth edition adds demodex
and most common forms of treatment
are lid hygiene basically and you could
um washing or cleaning your lids with
uh water massaging the lids etc etc
and the list of uh treating um
is like super long also as a side note
all my references are on the same slides
is trying to look for the same
information in the future
you can just try and google these
references and you would get a detailed
setup a set of information on what i was
and that can be super helpful sometimes
especially when you’re trying to read up
so the next big question is then
what is demodex blepharitis if this is
i think a little bit of a giveaway was
um my points to remember slide
wherein um i spoke about demodex
as a mite so demodex blepharitis is
blepharitis that involves demodex mite
types of demodex mites found in humans
now i specifically say found in humans
because uh there are other types of
just the fact that they don’t infest or
they are not generally found in humans
we will not be talking about
those these are the ones that are
primarily found in humans
the first one is demodex follicularum
which is approximately 0.4 mm long so
tiny you probably need a microscope of
look at them and perceive them and this
which is about 0.2 mm long so that is
one-fifth of a millimeter that is like
tiniest section on your regular ruler
so these are the two mites uh
that are infested that infest humans and
they have kind of like eight feet um
so they are classified as arachnids and
part where they feed and their thoracic
and the rest of the tail and the body
we really don’t um it doesn’t really
about their anatomical structure so i am
all of those facts and details and go
dive deep into their life cycle
and um because that will be helpful to
decide how to manage them
or what should the treatment be like so
the blepharitis demodex life cycle
of both of them are roughly they are not
different um and that is an adult
will take about three to four days to
uh the eggs will take about three to
hatch and form a larva and then about a
from there um those larvaes will become
again and then the cycle continues over
again so if you add up these numbers
it comes around to 12 to 14 days worth
which is a total of two weeks um and
one other important thing to remember
is what do they actually feed on and
they feed on the follicular and
glandular epithelial cells that are
in the eyelids and near the lashes
um also if they feed something they have
and their excreta may actually cause
of orifices and by orifices if you go
back to your eyelid anatomy it would be
my birmingham gland orifice where the
me burn comes out of or the um
follicles or the hair uh hair the hair
these are the places where they might
a little bit about demodex blepharitis
um wait if this is so common
and um they are there why haven’t
we seen them and like what what
what really is happening out there
so to go into the epidemiology um
among the first ones to identify these
uh blepharitis patients so he had some
blepharitis patients and he saw them
in these blepharitis stations we’ve
in almost about 100 years i think the
reference i could find was 1915
but they were primarily classified as a
you could get just like you can get
hair and because of that you can get a
lot of skin conditions like acne
and rosacea on your face etc uh that’s
where demotic smites had been
primarily classified as but in 1967
and around that time a lot of people
showed that these are also present in
and so they are ocular in nature the
uh findings are not very concrete
uh and i i will go into the details as
to why the prevalence range
is so so huge so we have a prevalence of
somewhere around as low as 29
so out of every 10 normal individuals
in three individuals and as up to as
a hundred percent uh depending on what
age group you’re looking at
um a lot of people are shocked to see
that or shocked to hear that
these um amazing looking tiny creatures
as i’ve fallen in love with them would
probably be creeping and crawling
on some of our eyelashes um as we speak
so yeah i know that is gross for some
yeah they are that commonly prevalent uh
however they are rarely seen under the
um one of the reasons being
that there are particular secretions
uh sebum that do not happen and this is
democrats might really like or feast on
they have seen less under the age of 16
um after we grow into a proper adult
um at the age of 17 18 that’s when we
the prevalence increases with age so as
i said the prevalence findings are up to
and some of the papers exclusively state
every individual would have um demodex
and since they are so common um there is
a lot of controversy in the field saying
that demodex might might just be
a part of the normal bioflora of the eye
they are not an infestation probably and
just see them normally because that’s
something like the gut bacteria that we
postulated like thesis of theories that
might be beneficial and not all that
and they affect males and females both
so yes it’s not that one gender is
in this case um the prevalence worldwide
across geographical regions
so far all the information states that
almost similar but since our prevalence
range is so huge already and we haven’t
that is something potential students
and future researchers can look into
to see if that differs from region to
but so far we believe that the
prevalence should not change
because there shouldn’t be any other
differences affecting these
demonic smite so how do you
get it like i’m pretty sure none of us
where does this my like how do you
and um excuse another one of my favorite
19 references but yes it spreads through
so probably your best solution is to
a six feet or two meters distance from
your closest other human being
uh but no that is not we are like that
is not something what we are
so yes but it spreads to human contact
it is it is understood or
it is hypothesized that um especially
and say we are about the age of 16 17
whenever someone touches our face or
especially i know my grandmother used to
love to pull my cheeks each time i would
and so i guess if i have demodex mites
um i probably say that that’s how i got
and then they have not left me ever
so yeah it stretched through human touch
if someone touches their face and then
that that’s a very common way to spread
it does it it is not caused or spread
via animals so especially dogs
have a condition which is quite popular
if you own a pet it’s called demodex
mandy i believe and it’s caused by
demodex canis as i said earlier there
are lots of types of demodex
and this is not spread via that so if
that condition it’s and if you end up
that it’s not the same um same might and
it’s not that your dog gave it to you or
you could give it to your dog
so yeah there is no worry over there
might be symptomless and is often and it
often is because i believe as
optometrists we all believe
that our lid is super hygienic and we
we have the least chance of having these
i have looked at some of my optometry
and a lot of us seem to have it and so
i believe that yes most of us do have it
but at the same time it is symptomless
and this is where the argument comes in
wherein it might be just a part of the
normal bioflora of the human eye
and hence we don’t face any symptoms and
it can also spread via uncleaned bed
if two people are sharing that then it
um one of the recent researches i found
um looking at how demodex can spread why
us the same microscope a lot of us uh
especially like things like in optometry
retinoscopes and ophthalmoscopes as
students we tend to share a lot of those
um and it might spread via that as well
um and it could spread through skin
for some um people it infects the skin
and if it is infected the skin for the
it might spread from their skin or
cheeks to their eyes so there have been
cases where that has been seen
so these are primarily the causes and if
you look at all of the causes
um there isn’t much we can do about uh
these like yes i can understand we can
bed sheets and pillow cases etc but
um human contact has is one of
as we can we are facing social
distancing we know how important it is
so i guess there’s not much we can do
about avoiding the causes so much
so to go ahead to understand what we can
do to manage this condition
i think it’s very important to see as
your patient show up as in the clinic
like what would you see when the patient
comes up with this condition
and since most of you must be thinking
wait i haven’t seen this common super
in the past um so i’m pretty sure you
it but no that’s probably not true most
demodex blepharitis in our lives in the
we just haven’t been able to recognize
let me give you an example of a case
all of us have seen um a demo expression
shows uh sorry a blepharitis patient
and um has mild form of blepharitis
probably in their 40s or 50s
and has itching etc the classic symptoms
and we treat them with asking them to do
like take baby shampoo and scrub it and
um and they’re fine after a week you do
a follow-up probably and they’re like oh
this is perfect like all is gone and i’m
fine and you look at the lids and they
everything’s going good and then um
you say the patient yeah you’re all fine
and good to go keep up with the lid
hygiene but other than that should not
after probably two or three months this
patient will come back to you again
and they they seem to have the same
and sometimes they’ll be like yes but i
already tried all of the lid hygiene
like i’ve not stopped it at all
and i’ve been continuously doing it so i
don’t know why i’m getting it again
and we and we are at our wits end
sometimes we might think maybe
the patient isn’t compliant and they
might have stopped for a while and they
i’ve heard other excuses like oh this
really oily skin and that is why they
tend to produce a lot of medium
and that’s what causes all of this and
things would be other explanations would
if you get dandruff on your head it’s
highly likely that it spreads from there
and comes to your eyelids
or i’ve also heard explanations so it’s
it’s super hot in the summer we tend to
sweat a lot and these kind of things
well if you look closer at all of those
if you’ve ever seen any i think you will
not any of those other reasons but
demodex blepharitis that is causing the
of that condition so going on to what
you would see in the clinical features i
think i pretty much described
what you would see but here are some
will help you the next time you see such
a patient to differentiate between
a common blepharitis condition and
something which is generic specialities
so you have to understand that demodex
primarily be diagnosed by signs
more than the symptoms because the
would um be anything that could um span
all forms of blepharitis dry eyes and
conjunctivitis and all of those so
signs are more important in this case
than um the symptoms that the patient
one of the most pathogenomic sign of
is the cylindrical dandruff like scaling
this image is primarily of um
cylindrical dandruff like scaling and uh
also known as clarets depending on which
part of the world you are
but what is important to remember here
is that if demodex is the cause then
your cylindrical dandruff
is primarily stuck very close to the
of the eyelid and um it’s almost
always just there and not at the other
of the eyelashes or it doesn’t really
off etc unless it’s huge in amounts in
which case it will fall off
but if you’re just looking at a
different blepharitis condition
seborrheic um probably caused by some
you will see um i know this is not a
very clear picture but you would see
that the blepharitis scales or
the the dandruff scales are spread
and not throughout the eyelashes and not
and just to go back quickly to the life
a life part that we study about demodex
blepharitis we know that they eat
um the follicular and glandular
uh epithelial cells and so
those are very close to the eyelids
and if they are eating there if their
food is there they probably reside there
in the follicles and if they’re residing
there they would excrete in the same
and that excrete would generally just
collect in these edges and not spread
and that is how we can somehow say
that this is the cylindrical dandruff is
primarily being caused by
demodex blepharitis instead of any other
also other than that as i already
that you have a lot other a lot of other
often there might be no symptoms at all
and sometimes symptoms would be like
itching dryness burning sensation
all the other symptoms that you can
anterior segment dry eye kind of
and symptoms would also be associated
blepharoconjunctivitis ty formation
meibomian gland dysfunctions
you might have had patients that come
saying um like you know every
six months or eight months they probably
a chileasian or internal external
cordulum as we like to call them um
and these might be just sometimes these
are just the associated condition
to the primary condition being demodex
blepharitis not always but sometimes
they are just associated conditions
and we of course treat these associated
conditions and they go away
um but again after a few months the
patient comes back with another similar
and we are like oh yeah this is a
he’s going to have this for a long long
time probably an allergy or something
but it might be wise to look at the
if they have demodex nephritis and now
all the clinical features that we should
i think it is time for us to um
to really understand how can the
or what is the ultimate test that you
to say okay this patient has demodex
refrigerants and i should start treating
accordingly um well good luck there
because there is no official test for
diagnosis though we’ve known for demodex
in the eye for 50 years the primary two
are one they are so tiny that for a lot
of those 50 years most of us
didn’t have um equipment or enough
technology to actually be able to
um and then you’d be like but well
in most parts of the world like 20 years
ago or 30 years ago it’s not the first
someone saw split lamp in this century
part is that we don’t have any official
test or clinical diagnosis set up or any
so most of the practitioners and
probably even our faculty
um that’s why we weren’t taught uh in
and and i’m so sorry if i was sleeping
i wasn’t um is that we are not aware of
existing and we’ve been treating just
the symptoms that show up
and for a lot of us it solves the
because it might just be that demodex is
flora and fauna one of the reasons that
is that um even though a lot of people
argue it might be a normal bioflora
the thing could be that it is
normal bioflora until it is in a certain
but if it starts growing in the
uh super quickly that is when the
that is when it starts causing all the
some of the controversies that they help
eat or digest dead cells around the
and get rid of those dead cells and
the orifices so that our glands don’t
and then the cylindrical dandruff
probably just falls off or we clean it
but at the same time the other side says
that well that could be true until a
certain limit but if you have like
um say 10 demodex might feasting on one
follicle then they probably start
itchiness and they might start eating up
all the good cells that we need
and going back to the diagnosis uh
causten in 1967 came up with his own
um to diagnose this but if
i’ll explain i’ll walk you through it
and you will realize that this is not
something you would want to do in your
and so his method was to epilate four
from each eyelid that would mean on four
from the upper left four from
the down left and four from the upper
right and four from the down right
then to place them on a slide the slides
that we used in biology probably in 12
etc to place them on those slides add
peanut oil and apply a coverslip on that
then to place this slide under a
microscope and count the number of mites
and that seems extensive one when i
i don’t have a light microscope in my
i don’t think my patients would be super
happy if i started plucking like 16
eyelashes from their eyelids they would
regardless of how bad their demodex
and so convincing patients to do that
so in 2005 gao came up with
a sort of modified version of it um
and he suggested to epilate like two
uh once one from each half of the eyelid
so to as so as to cover the whole eye
completely this cuts down the total
number of flashes from 16 to eight
but again his procedure was to place
and now i guess we had access to saline
was to add 20 microliters of saline
and or use hundred percent alcohol if
there is a lot of dandruff or
the cholera as we like to call them
stuck to break up the cholera
and place a coverslip and again count
these mites under a light microscope
in a tertiary eye care center that might
but not in your regular clinic where
you’re most powerful tool probably is
so i think murphy came up with this high
guideline just a couple of months ago
very recent data a very recent
um he suggests that choose an eyelash
or without um color it so your primary
goal should be to choose one with uh
around it with forceps you don’t need to
epilate or pull out the eyelash but you
the lash four times clockwise and
um and i have tried this on a slit lamp
really don’t have so much space to
um the eyelash but yes that is what the
um his criteria was and then
to count the number of mice associated
on the slit lamp bio microscope so
you’re not pulling out the eyelash
you’re just looking at the mites on this
now something you should know about
these mites is that there are eight feet
that they have along with that very
razor tooth mouth that they have these
like attach themselves super close and
to the follicles and eyelashes
and that is what causes them to stick
onto there and they are so ins they are
kind of burrowed into our follicles a
and that’s why we just don’t see them on
the slit lamp as it is and that’s why
procedure of rotating the eyelashes
um and i think rotating the eyelash
eyelashes kind of disturbs them from
and wakes them up and they wriggle
around or probably move out thinking
probably there is an earthquake on the
eyelash and they need to find a new home
and that’s when you catch them catch
them red handed or in action
i also looked at what the new kanski
kind of a mix of all of these versions
and again as i said there is no
official test for diagnosis but you can
um any of these if you have the
and you can see what works best for you
um list is kind of the best so kanski
mentions using a slit lamb biomicroscope
with 16x or higher magnification
and to get rid of probably all the color
with forceps to gently rotate or move
side to side the eyelash for five to
this is really long uh in some patients
seen that they come out super quick um
i think instead of rotating moving the
is so much more easier on the slit lamp
and the last one is if one or more mites
if that is that mice do not come out and
determine if there is a demodex
then you epilate the lash and perform
so this would finally be the ultimate
i think once we spoken about what
technique you want to use
since there is no official guideline
for whatever you want to use um until a
but until then yeah try your best to see
i think murphy would be the easiest one
to do it without disrupting your
and what we would actually see is and
this is again a picture from
kansuki because it’s very hard to catch
um so this is a demotic smite
um on the image over here with the arrow
and this image was clicked two seconds
later and you can see that might has
moved from there to there
this is what you would see the mic comes
out from the eyelash follicle
and is running um in some direction
going around and they are super quick
like they are tiny in size no doubt but
fast they can really really move fast
you it is hard to if you’re looking for
them it is hard to miss the movement
um so this is what you’re looking at
on the slit lamp and this is probably
for diagnosis to see the demodex might
unless you epilate the lash and watch it
so once you’ve done this um
if it is so commonly prevalent it would
decide whom to treat and whom not to
everyone get a treatment because it is
that depends on the symptoms um as well
if the patient is showing some symptoms
yes you should go ahead and treat them
if it is not then i would resort back to
not disturbing something that seems to
be in a perfect harmony or balance
naturally so going back to that um
there is a grading scale that murphy
um his method as i said is quicker
and less painful than the other methods
he also found that the mean of
1.45 mites per lash was detected by his
method as compared to the appellation
method where the mean of zero point
mites per lash was seen well this data
hasn’t been verified strongly yet but
if it is true then probably his method
superior than the other methods of using
so quickly going over his uh
grading scale is over here you can see
in the table that there is grade and the
you have zero mites uh sorry you have no
mites which would be grade zero
you have grade one where it is mild
um and it is one to three mites per
follicle so basically a one lash per
follicle so if you disturb one lash if
you see one to three mice
that is somewhere um acceptable or
but if it is it is moderate if you see
four to six miles per follicles
which is um which is the scale where he
where murphy says that more than or
is abnormal so beyond this um anything
severe is more than seven mites and
beyond this anything you would want to
um to see if and especially want to
to see if they have any uh symptoms
so what treatment are you going to use
now we know how to diagnose it and we
want to go ahead and make sure that we
these patients again as along the lines
of diagnosis there is no official
guideline so far out there for
um and i know some guy some um
etc are under in process of preparing
certain guidelines for the management of
but since it’s been improperly diagnosed
uh we don’t have a lot of information
and there is no official guideline
but current strategies primarily any
blepharitis i think this is our to-go
currently is improved eyelid and face
clean eyelids um with all different
scrubs etc then frequent cleaning of red
pillowcases and hot water this also
and this might alleviate the symptoms
reduce the load of demodex might and
may bring it down to like the normal um
level or the bioflora level and your
patient might just be fine
but um and treating any associated other
conditions of course that would be our
primary concern because that’s what
so these are our current strategies and
if your patient is fine with these
okay and if there is not something you
want to do more for this patient at this
or we feel yeah if it is okay fine but
if this patient comes back after a few
seen this patient come back recurrently
which i believe most of us have
then you want to proceed with managing
so there are two options that come up
um if you look up in the literature and
first one is intense pulse light um
and i’m not going into a lot of details
um this is like a pen kind of machine
that is used in skincare clinics
especially to get rid of acne marks etc
and as the name suggests it’s a pulsed
light so there are pulses of
one particular wavelength of light that
given to the skin or that area and that
potentially heats up that area and it’s
not burning the skin or anything like
it just heats up the area and it
kills the might so there is one study in
that proves that this is very much
the problem is it is expensive a lot of
us won’t have it available
and you could try and look for a
skincare clinic around you if you want
but yeah again it is still expensive and
to apply it like patients can’t do this
or you can’t do it at a clinic you need
someone who’s been trained in this skill
but the second one is a tea tree oil
and this as compared to intense fells
is cheaper easily available and you can
but there are a lot of caveats and i
in this image on the right you can see
and again in the reference below if you
want to look at all the molecules that
have been identified for tea tree oil
um you can check the reference out
and tea tree oil basically comes from an
alternifolia shield i believe so
these come from the leaves of those
plants and now they are commonly
available in a lot of places they become
natural treatment just like manuka honey
for a lot of conditions and the reason
these all components or compounds that
we do not clearly understand what they
do but these are their concentrations
and i wanted to show this particularly
because some companies are manufacturing
for treating demodex which says terpenin
for all and you might be like okay this
is not treasury all this probably won’t
help but this is the main component
uh which is present in the most common
and some of these other components also
these have been identified to be the
a demodex um so yeah you want to do a
little bit of research if you find a
product at your local pharmacy
to see if it’s actually helping uh there
because there are a lot of companies
that are looking into this currently
um so what are the caveats of
using treaty oil why haven’t we started
using it commonly and why is it not
uh yet apart from the fact that people
have been struggling with a lot of other
treatments if you go online there is a
um including pilocarpine etc to treat
uh this has been the most effective and
uh that is where the review that i did
wherein of course there aren’t many
studies but and this is not
statistically this data is not
statistically significant
this paper is undergoing peer review so
hopefully it will be published anytime
um on this platform so we probably get
emails about that i guess
um we found three studies with strong
evidence or good evidence
even though this is not any signifi
statistical significance to
treat this um the studies were compared
to all the other groups so i think zang
2019 over here was compared
and it used intestinal slide and coup
um i believe did not use a treatment at
all on the other hand and this one um
the nct trial also did not use any other
um except for zhang 2019 with intense
false light we see that the other two
fared very well so instead of not doing
or just prescribing lead hygiene uh
sorry coup 2012 had laid hygiene as
for both their true group and the
and the non-trial group i think it is um
beneficial to prescribe this and see if
um so this were the primary results the
review goes into a lot of other details
most of it is not clinically relevant
and hence i’ve kept it out of this talk
um so your treatment plan what should
you have to remember that when i say tea
tree oil you just do not go to the
buy tea tree oil and apply it on lids uh
application of tea tree oil in low
control low concentration
that is the earth’s most significant
because in high concentrations tea tree
the eyes burn and um the burning
sensation lasts for like a lot of time
uh if it ever happens um splashing water
on the eye is your best way out
so yes we do not want to one give
access to high concentration because
they might forget or they don’t know
that’s why patient tree patient
one of the most important factors so
there as i said there are no guidelines
these are some rough areas that you
use as templates one is in clinic
regimen these are both possible um in
clinic can go up to like 50
concentrations so basically you mix up
half tea tree oil and half some regular
that is not harmful to the eye and you
apply this so you clean the eyelids
and then you ask the patient to close
uh take a q-tip or a cotton tip
applicator and you scrub the eyelids
uh properly for say five or six
times or a couple of seconds both for
and lower eyelid and for both eyes and
this can be your clinical management
um one the thing i feel is that this
on a weekly basis and then you can give
the patient to do something similar for
and at home has a range from like 15 to
concentration and you’re free to decide
land with this at home treatment and the
at home probably twice a day and this
help reduce the or kill the mice
effectively there are commercially
available scrubs depending on what part
i know some names in u.s but i didn’t
want to put any brand names in here
so look around and see if there are any
available scrubs or ointment
and that might be more easy for the
patient to use rather than this
tea tree oil when they would dip the
cotton tape in the oil etc
patient education and constant
um and this is where some of the studies
this treatment tends to fail is patient
or there aren’t constant follow-ups a
recommended duration of treatment is one
to three months one month because that
includes two cycles of demodex might
and um that is the most um
that is the least amount of time
required to get rid of most of the mites
otherwise they would just proliferate
again and um start causing the same
and if the patient comes up comes back
and you still see some mites it’s
recommended to go all the way up to
if at that point you’re still seeing
mice or if the condition is not
resolving it might be something else and
you might not be treating the right
um and patient compliance is a key
i believe up to some of the studies show
causes eradication of demodex mites in
of the patients so if your patient is
twice a day for seven days a week and
the patient comes back next week
and the patient says oh i’ve done it
like almost all of the days twice a day
then there is highly likelihood that at
40 percent of those patients you treated
uh be would have no demodex mice at all
but if at the same time if the patient
is like yeah i did it twice a day for
the initial day or two and then i forgot
completely because as soon as the back
load will go down their symptoms if
like gone and this is a classic case of
the symptoms gone i don’t need the
um and the demodex mites will start
working again and probably the patient
will come back to you in a couple of
months with the same problem
so yeah patient compliance is a very
um last is what should we record
this is more in terms of research um
or to see how your patient is
you should always record vision but
vision does not change a lot
anterior segment signs and uh symptoms
if there are any like redness etc some
patients do show up with that
and we might commonly do that when we do
slit lamb but we classify it as
but this would be a big segue one of the
things that the researchers have been
if you ever plan to share your data or
publish is the osdi score
um and which is ocular surface disease
it’s commonly available online you just
need to put osgi score it’s a very short
seven or eight questions if i’m not
wrong and the patient fills this out
and over time researchers have seen that
score changes and the last is
compliance it is very important for you
especially as a clinician even if you
is to see how compliant the patient is
because you might feel that this is not
and you might try to do some other
but all it could be was that the patient
each time if you see them weekly or
monthly each time you want to ask
how often did you use the treatment and
that would probably give you a rough
as to where you should head further
whether patient re-education is needed
so that they become more compliant
or if they have been super compliant
then we might have misdiagnosed this
um and we are trying we should look for
at that point and treat that
so to summarize uh frequent testing for
sure we all see blepharitis patients all
the time and since the prevalence is so
i think frequent testing for any
suspected individual or groups of
would be very helpful since it’s a very
easy test would probably take seconds on
it’s high prevalence hence uh there is
because i know it can be hard to learn a
from scratch without any guidance or in
but the prevalence is so high that if
you start looking for these
in most of your patients i’m pretty sure
you will be on top of this
very soon um keep a lookout for updates
on guidelines because the community is
riled up about not having a proper
and so guidelines would be soon coming
and do not be afraid to prescribe
i know it’s toxic and people get scared
at the point oh it’s toxic
i’m not going to do this i don’t want my
patients complaining or coming back
saying your eyes are burning etc
um yes it is toxic but at the same time
you have to make sure that you’re not
giving them 100 concentration
um and educating them that they do not
and buy it off the counter and use it
be harmful to them you need to make sure
what the concentration is
but it’s already been used in the hair
care and skin care industry
very frequently especially to treat
dandruff and things like that
so it’s easily available out there and a
have been using it as a natural remedy
um for these conditions so
i think it’s we buckle up and use it for
treating demodex blepharitis as well
and we should not be afraid to do do
one of the things that i came across in
the cost in 1967 paper and i would like
is if especially when performing slit
lamps sometimes some patients are
really uncomfortable and they complain a
lot about even the lowest life settings
and question says this while doing
democratic smite if obnoxious attitude
is exhibited by the patient while trying
nothing is more humbling than to
announce madam you have mics in your
and um this is a blanket statement you
can confidently use this for any other
because you will be statistically um
probably right that the person has mites
so with that i would like to acknowledge
dr andrew parker my mentor
um dr jimmy lee who actually did a lot
and a lot of work in the review that is
um cochrane i and vision team they were
super helpful in walking us through the
and uav school of optometry for
all the help and progress i’ve made so
uh with that i would like to thank ools
all of you for attending this seminar i
this was super helpful and once the
or you start seeing patients this is
something you would keep in the back of
and uh start looking actively and
so that this this condition can be much
treated and pro and we will lose all of
um those recurring blepharitis patients
we’ll be able to provide relief for them
uh i guess that’s the end of my
if there is time for questions i will
okay so thank you thank you very much i
it was a very wonderful presentation and
to be very honest when you gave me the
topic my thoughts were the same
thoughts you had with your supervisor
that what what’s this topic you want to
i actually went by googling the topic to
so i don’t think you were sleeping in
the class you’re pretty much awake
for the for your ocular disease class i
am pretty much sure about it
so let’s take some questions we have two
uh one of it is yes you mentioned about
the the tea tree oil which can be used
as the management so should we actually
consult the dermatologist before giving
um one there as i said there are no
um and tea tree oil is a natural product
there is no harmful or long term harmful
the most i have seen happen is
and like burning sensation for a short
duration of time and if you wash it off
there are no contra indications so far
but yes if the person on the cautious
is undergoing some other skin treatments
there might be some patients who have
nephritis as well as some skin problems
then it would be wise to consult with
their dermatologist to see if it doesn’t
interfere with that treatment
but other than that it is safe to use as
uh especially in low concentrations
okay and any tips on how would you
explain the patient in layman terms
about this particular condition
i mean apart from the court you
mentioned is there anything else you
especially in my experience one of the
really get scared about or would reject
is when we mention mites and we are used
but we expect to see them when i look
in the mirror there are some techniques
instruments being developed with phones
to try and see it or diagnose it with
phones etc and cameras etc
but um they aren’t advanced enough and
but um i think educating them
to show that this is something very
and the prevalence is super high so they
and um that it it like probably
a lot of people have it and it’s okay to
have it i think that is super helpful
in pacifying them um and helping them
understand that this can be easily
and it is not something that they should
be scared of especially with the stigma
the word of mites that’s right and
yes you mentioned about the range of
percentage which ranges from five
50 percent uh which is a bit larger
range so any comments on the minimum
would like five percent do the work any
clinical experience on that
so uh this is one of the things that um
the whole point of my review is to try
and see what’s out there and where we
and um as malan has clearly asked
we definitely need more information out
planning to do a phd masters or even a
it would be a great topic to look into
there isn’t clear guidelines or
information as to what is the optimum or
these are the things that people these
are this is the range that people have
so we don’t know even if 55 would be
good but no one has ventured
that far at least not documented
literature and it would be best
to avoid until we know um the toxic
effects beyond 50 at least but
up till 50 it has been used successfully
um unfortunately i do not have the
short answer for that currently yeah so
and i think you mentioned in the talk it
could be taken up as a research project
by the upcoming optometrist who wants to
pursue higher education to check
uh the various concentrations like they
do in myopia control for entropy they
and 1 so something of that sort can be
thought about in in the effectivity of
treatment modality yes next question
yeah the next question is since the
you know so high uh should we start
blepharitis patient as demodex rephritis
or what’s your take on that that’s an
start with the worst ones or the most
um but not all of them because sometimes
the whole idea of the treatment
currently is to reduce the demodex mites
even if you even if you end up
it is highly likely that they will catch
them again from someone else
um in their vicinity um so
i think what is best going forward is to
if the most recurring or the your worst
case scenarios which are not being
treated is to start treating them with
but not reading all their cases with
this because finally the ultimate goal
which can happen not very effectively
but definitely can happen with
uh just lead hygiene etc and once we
better guidelines and more information
safe to use then yes of course at that
yeah and any disadvantages of
thermal pulsating treatment for this
condition so unfortunately in
my research only one study
only one significantly strong study that
the that was that was the only study and
cannot confidently say that there might
be no disadvantages the study does not
uh especially for the patient and the
but yeah the other disadvantages are as
it’s not easily available it’s expensive
but yes the research is lacking in that
so yeah i don’t know if there are any
particular disadvantages but it’s been
used extensively in skin care
and whatever i understand from there is
aren’t any significant disadvantages of
treatment okay and the treatment
normally works the same for both of the
demodex mites what we have
learned today yes as i said initially
uh that the treatment is same for both
the mites uh and that’s why i did not
uh so far at least um we do not
if there is any difference we do not
understand that yet and that’s why i did
into the anatomy and the pathophysiology
of the effect of both mites
dermatitis follicularum primarily
affects the anti it’s primarily the
cause of anterior blepharitis
and demodex brevis is primarily the
of posterior blepharitis but yeah
for us currently the treatment is uh
equally effective and we do not
understand if there would be a better
or better way to treat one over the
yeah it’s that’s what we have for now
okay and any side effects of the t3 oil
on the oculus surface or any
complications in general and would they
i wouldn’t say they would so
once the review gets published you’ll
see that again data in this area
is significantly lacking the studies
that are published in the review
do not really speak a lot about
severe complications they do some
that patients feel uncomfortable burning
and having used uh tree tree on myself
to try and see how it feels it does burn
if you end up applying it to the cornea
by mistake but apart from that um
i haven’t seen any long-term effects but
again no one has really tested putting
of the concentration in the eye yes it
and it might have a lot of long-term
effects and hence the guideline limits
to or at least so far people have
limited the use of it to the
concentrations that i mentioned
and do the number of months that i
mentioned so it’s not a lifelong
but at least one to three months and it
okay and just just let’s take one last
question as you mentioned about
does this mites make conjunctivitis or
inflammation is worse or does it only
so what happens is these mites feast um
it’s it’s a it’s a bad cycle of problems
so one they these are feasting on all
your good cells in the eye that are
producing the anti-inflammatory factors
etc like your medium and um
so these mice are feeding on that one so
all those cells so you’re going to have
factors that you need and on the other
uh stuff that might be toxic to the eyes
most of the times especially in
it has been seen that this
has been primarily the cause and that
a secondary outcome or a secondary
so yes this does make informations
worse um and we we keep on trying to
treat the secondary associated disease
um and we haven’t been able to identify
so yeah that is um that is definitely
okay so yeah one last question we just
popped up i think we’ll just take one
any chances of contact lens wearers to
suffer from this condition
or is there any influence of contact
yes yes definitely of course the
as i said no one has looked into it but
like it has been seen that people using
not cleaning their lids etc that is
and then because of some imbalance in
uh homeostasis of the environment uh
it gets affected so yes contactless
sometimes um especially with uh the
first dues and all they are looking into
where in some of the dryness we haven’t
really classified all the possible forms
dry eyes and some think that some of
um dry eye patients which we aren’t able
to understand what is the cause
um it would it could be that demodex
blepharitis is the cause so
um yes definitely screen and look for
this in your contact lens wearers who
suffer from itching etc or even dryness
so as i said the symptoms are very vague
but if anyone comes up with those
um allude to any other reason then it is
no harm to have a quick look on the slit
lamp to see if they might have some
yeah i think the main important thing is
follow up them and look for reoccurrence
you know since we don’t have much of
evidence on the diagnostic tests and all
so at least look for your occurrence and
at least see if people are having
you know recurrent and not getting
treated treat them as having demodex so
that at least you are doing something
so thank you very much uh ku for you
know a wonderful talk i think
all of us definitely enjoyed uh learning
something new which was not there in
our time of kanski and something which
now being thought of a lot thank you
once again from the whole team online
thank you thank you so much everyone
and hopefully you will have a great rest
yeah thanks so it’s a sunday morning
the whole day is ahead yeah some of the
parts uh i mean here we are almost off
to bed 10 45 here in in malaysia i think
so i would like to wish those who are
happy happy eid ramadan kareem to those
who are celebrating today and
i would like to wish those who will
celebrate tomorrow in some parts of the
world a very happy eid as well
same here samia thank you so before
yeah before we go i just like to share
my screen we do have uh sessions planned
weekend so let me just share my screen
let everybody know so yeah there you go
so next week we have dr nitesh bharat
and he is going to talk to us about
in in practice so please tune in next
uh saturday 6 30 p.m indian time
in the evening and 9 pm malaysian time
and see you all again next week until
