
Age Related Macular Degeneration
Age related macular degeneration (ARMD) is a disease of the macula or one’s central
vision. An early sign of ARMD is distortion of vision. For example, straight lines appear
wavy or tilted. This distortion of vision is called metamorphopsia. In more advanced
ARMD, patient’s will report loss of their central vision that appears like a black spot.
Many patients with ARMD continue to have unaffected side or peripheral vision. ARMD
runs in the family and has a genetic component. Individuals at higher risk for ARMD
include fair skinned, blue eyed individuals, smokers, and individuals with high blood
pressure.
Two forms of ARMD exist: 1. dry and 2. neovascular or wet
Annual dilated comprehensive eye evaluations will help detect early signs of ARMD.
The risk factors for macular degeneration are
- age
- light complexion / light irises
- family history
- sleep apnea
- metabolic syndrome
- high blood pressure
- high cholesterol
- diabetes
- obesity
- high myopia
In early diagnoses of Dry ARMD, and in all patients, the recommendation isto stop smoking, start consuminga diet high in green leafy vegetables such as kale and spinach, and wearing UV protectingsunglasses when outdoors. Special vitamins may be given to high risk patients called the AREDS II formula. The AREDS formula vitamins have been specially formulated to help reduce the progression of ARMD. We offer a special formulation that guarantees that it will increase your antioxidant level. If you are a smoker or have a history of smoking, tell your doctor as the formula may need to be changed custom for you.
Aside from comprehensive eye exams, patients can monitor the progression of ARMD at
home. The Amsler grid is an important tool to monitor for changes or development of the
disease.
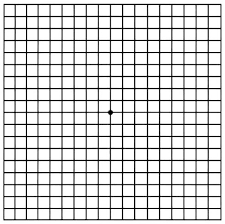
Instructions:
Cover one eye and stand arms length back from the grid.
Focus on the center of the grid and pay close attention to grid in your side vision.
If the lines look distorted, wavy, or even missing, report this to your doctor right away.
Monitor for changes, new areas of waviness or distortion.
Repeat with other eye.
Wet ARMD is a more severe form of the condition. Treatment such as injection of
special medication or lasers may be required in order to help prevent vision loss. Patient
with wet ARMD will be followed more carefully and more often by their eye doctor.
AMD
Association for the Blind
Vision Loss, Update Age-related Macular Degeneration
Most of us are aware of the changing demographics in America. People are living longer and diseases of aging are becoming more common and debilitating The prevalence of severe visual loss from AMD increases with age, and most patients with AMD-caused visual impairment are in their 60s or 70s. In the U.S., age-related macular degeneration (AMD), formerly termed senile macular degeneration, is the leading cause of severe and irreversible loss of central vision in people older than 50. It is the second major cause in 45-64 year olds Some features of AMD can be detected in up to one-fourth of those over age 65 and in one-third of those over age 80. Macular degeneration, formerly termed SMD, affects as many as 30% of seniors over 75 Slightly over 2% of those 65 years of age or older are blind in one or both eyes from AMD. Fortunately, however, most cases of AMD do not result in serious visual loss. Although there are various definitions of severe visual loss, a decline in visual acuity to 20/200 (seeing only the big “E” on the eye chart) or less is commonly accepted. . Low Vision is defined by different organizaions in different ways. CAUSES OF AMD Epidemiologic data indicate that individuals with low plasma concentrations of carotenoids and antioxidant vitamins and those who smoke cigarettes are at increased risk for age-related **macular** **degeneration** (AMD). Numerous conditions lead to this as a common pathway. Infections such as histoplasmosis, hereditary diseases such as retinitis pigmentosa or nystagmus or albinism or optic neuropathy, ambylopia, congenital malformations, trauma, retinal detachment, macular holes, cysts or edema, Diabetic retinopathy, Macular degeneration, Glaucoma are some of the more common diseases. Cataracts and corneal failure are quite common but they generally lead to a reversibile cause of loss of vision. We will focus on the irreversible causes of vision loss and the latest research and developments. The most sensitive part of the retina is the macula, an area about one fiftieth of an inch across located in the center of the retina at the back of the eye. The macula is the re,lon of the retina most densely packed with Z:> cones, the most sensitive receptors of light. Central vision and detailed vision depend on an intact macula. If macular function is lost, activities such as reading, normal-sized print are impossible unless low-vision aids are used. No matter how hard one may try, reading small print out of the corner of the eve is impossible; at best, peripheral vision allows one to see the big “E” on an eve chart. The cause of AMD is unknown. Numerous risk factors have been identified in cluding heredity, sex (females more commonly), light color eyes, hypertension, cardiovascular disesase, smoking, phototoxicity and aging. Risk factors, in addition to aging, include: hyperopia (farsightedness); cigarette smoking; a light iris color; and a positive family history. Benefits of treatment have been shown in only a minority of patients, though many low-vision aids are available to help patients go about their daily activities. There are two forms of AMD: non-neovascular (also known as nonexudative, atrophic, or dry) and neovascular (exudative or wet). About 90% of people with AMD have the non-neovascular form, which is associated with aging and is characterized by a breakdown or thinning of the macular tissues. Although there is no way to prevent or reverse this form of the disease, the changes occur slowly and may stabilize for periods of time. Neovascular AMD is the more serious form of the disorder, and it is the primary cause of AMD-related visual loss. It may develop at any time in people with non-neovascular AMD. Visual loss from neovascular AMD results either from the growth of new blood vessels (called neovascularization) in the choroid layer of the eye or from the subsequent detachment of the layer of pigment epithelial cells just beneath the retina. These newly-formed blood vessels tend to leak Cataract Removal to Diagnose and Treat Retinal Disease Cataract surgery is sometimes recommended to provide an unobstructed view of the back of the eye and aid ophthalmologists in the diagnosis and treatment of suspected retinal disease. To determine whether such surgery is in fact helpful, researchers from the Wilmer Ophthalmological Institute at Johns Hopkins monitored 17 patients, average a-e 67, who had cataract surgery in order to evaluate the retina. A total of 20 eves were treated; 16 were known to have diabetic retinopathy and four were initially diagnosed with neovascular age-related macular degeneration. The researchers found that cataract removal did benefit patients with possible retinal disease. Cataract surgery permitted accurate evaluation of the severity of the diabetic retinopathy in each of the eyes with known retinopathy. Six of these eyes underwent laser treatment-which would not have been possible before the cataract surgery-and visual acuity improved (meaning that patients were able to read at least two more lines down on an eye chart) in five of them. Even when treatment was not found to be necessary, cataract removal improved vision for the majority of patients. Cataract removal also permitted a more accurate diagnosis in all four of the eyes thought to have neovascular age-related macular degeneration. Although these cases were not treatable by laser therapy, cataract surgery nonetheless improved visual acuity in three of these eves while the fourth was unchanged. ,AMERICAN JOURNAL OF OPHTHALMOLOGY VOLUME 118, NUMBER 4 October 1994 The retina is the light-sensitive layer of nerve tissue that ,lines the inner eye. It is made up of millions of tiny nerve receptor cells called cones and rods. Light rays reflected from an object are focused by the cornea and lens onto the retina, triggering the cones and rods to send responsive impulses through the optic nerve to the brain. Cones are primarily, responsible for daylight vision and seeing detail and color; rods are more important for seeing in dim light or darkness. The most sensitive portion of the retina is a small area located at its center, called the macula, which is responsible for central vision and seeing fine detail ‘ In the middle of the macula is a small indentation-the fovea-that contains the highest concentration of cones, making it the area of most acute vision. When you look directly at an object, the light rays focus onto the fovea. Age-related macular degeneration (AMD) impairs central vision and the ability to distinguish fine detail-visual functions necessary for such activities as reading and driving because it damages the macula. Non-neovascular AMD is caused by a gradual deterioration of macular tissues, and usually progresses slowly over the course of years. In some cases this condition may develop into neovascular AMD, which involves the growth of tiny new blood vessels beneath the macula. These fragile vessels leak fluid, causing severe destruction of the nerve tissue in the macula. Fortunately, this condition may be slowed or halted in some patients with laser photocoagulation. and exude fluid (including lipids or fats) under the retina, hence the old name, “exudative” AMD. Neovascular AMD can be further classified by the location of the new blood vessels (and the site of fluid leakage) and whether the extent of new vessel formation is poorly or well demarcated. The location is described by the proximity of the neovascularization to the fovea, the I central and most sensitive part of the macula. New vessels most distant from the fovea are termed extrafoveal; those at the fovea itself are called subfoveal; and vessels in between are named juxtafoveal. An overgrowth I Of connective tissue, which accompanies the neovascularization, produces the scarring that is responsible for loss of vision. Left untreated, severe visual loss occurs in three years in about 60% of eyes with extrafoveal neovascularization, in two years in @0% of eyes with either )uxtafo – veal or sl”–oveal neovascularization, and in two years in 40% of eyes with poor :demarcated new., vessels. Moreover, w@en neovascular AMD occurs n –,e eye, there is a 20 to 60% chance that the other eye I I 1 II become slml ., @,-Iy affected within the next five years. w SYMPTOMS OF AMD The symptoms AMD are an other-wise unexplained distortion of objects and a loss visual acuity that can be mild and develop gradually (non-neovascular) )r be severe and occur in a matter of days or weeks (neovascular). A Coyness or haziness or a blank spot may appear in the area of central vi i Is”,n, words may be blurred on a page, and straight lines may appear to have a kink in them. Objects may seem to be smaller than they are. Color vi is@,)n may become dimmer, since the receptors involved in color discrimin:–,;ion are most dense in the fovea. Visual distorti load can be detected by self-monitoring with an Amsier id, which is a b(,4 ubdivided into smaller boxes by a series of cross,o,ri I I connecting perpeii,iicular lines. Patients hold the grid at reading dis- tance and fix one xe o,, its center (with the other eye closed). Indications of early sta@@s of AMD include minor blurring or wavy or distorted lines. M(,re advanced cases lead to gray areas or blind spots around the center (,f the visual field. The Amsler grid alone, however, is not a reliable Iindlic;,for. Because many patients may not notice gradual changes in vision, they are advised to monitor their vision in several ways, such as durin:,, reading, while watching television, and by noting the appearance of v;i,ious objects. DIAGNOSIS OF AMD A diagnosis of neovascular AMD is suspected when an individual notes the onset Of new symptoms and an eye examination shows an exudate (fluid deposit) or hei,iorrhage in the macular area. The diagnosis is confirmed by fluores,,.in angiography. This test must be performed quickly and the results interpreted promptly because the disorder can, within days, cause ” 1 (@versi ible damage. Non-neovascular AMD is diag- nosed when the do, or observes certain abnormalities in the macula during an ophthaim,,,;co – pic examination. Fluorescein anglography generally is not required. Angiography Fluorescein (a special dye) is Injected into a vein in the arm and photographs of the retina are taken as the materlai circulates through the I blood vessels of the eye. The light from the camera flash s passed through a blue filter; Lile resulting blue light stimulates the fluorescein to emit a vellow-green ight from the vessels in the retina and chorold and Dark Green Vegetables May Lower Risk of AMD Additional evidence that spinach, collard @reens, and other dark -reen, t, Z3 leafy vegetables rich in carotenoids mav lower the risk of age-related macular degeneration (AMD) was published recently. In a study involving 356 patients with advanced AIMD and 520 patients with other eye diseases, researchers found that a high intake of carotenoids reduced the risk of developina AMD bv 43%. Carotenoids, pi-ments in fruits and ve-etables, have an antioxidant effect, and thus may help prevent certain diseases. Specifically, consumption of the carotenoids futein and zeaxanthin (found in spinach and collard @reens) was associated with a “dosle-dependent” reduction in AMD risk-in other words, the more of these particular carotenoids contained in a person’s diet, the lower his or her risk of AMD. Taking supplements of vitamin E, vitamin C, or multivitamins did not change AMD risk. There are manv explanations for how carotenolds might help prevent AMD. One possibility is that the outer lavers of the retina are rich in polyunsaturated fatty acids, which are prone to a type of damage prevented by antioxidants. The macula itself contains futein and zeaxanthin, and other studies have shown that these carotenoids act as a filter to prevent harmful ultraviolet light rays from reaching the macula. Although further studv is necessary to confirm the @i.k between carotenoids and AMD, there is likely no harm in consuming as many dark @reen, leafy ve-etables as possible. z’ JOURNAL OF THE AMERICAN MED- ICAL ASSOCIATION VOLUME 272, NUMBER 18 ivovember 9, 1994 V I S I 0 N 0 1 S 0 R D E R S E 1 9 9 5 from any fluid that has leaked from damaged vessels. This procedure is associated with some risks (death in about 1 in 225,000 patients and serious medical complications in 1 in 2,000 patients) as well as a small chance of nausea or @omiting, but it is essential to prove the diagnosis and to identify the sites of neovascularization. A newer test, indocyanine green anglography, which uses a similar procedure but with a different dve , is sometimes employed if the fluorescein anglogram does not adequately delineate the abnormal vessels. TREATMENT OF AMD Unfortunately technology and medical developments are laging behind in the treatment and cure of these disorders. Last time we talked we discussed submacular surgery. With fine forceps a neovascular complex is carefully disected from the subretinal space. If there is profound bleeding beneath the retina, before clot organizes it can be evacuated with surgery. Still the mainstay of therapy is laser surgery. Tissue plasminogen activator (tPA) (250 micrograms/ml) was used to facilitate removal of submacular thrombus in 15 patients. ** Vision improved in 13 patients and remained the same or deteriorated in 2 (mean follow-up 11 +/- 4.9 months). Well-defined subretinal neovascular membranes were identified in 2 patients and occult neovascularisation suspected in 2 others. A cataract developed in 1 case and retinal detachments in 2 others; all were treated successfully. The poor visual prognosis associated with submacular haemorrhage may be obviated by the use of the technique we describe. Laboratory data show that carotenoids and antioxidant vitamins help to protect the retina from oxidative damage initiated in part by absorption of light. Primate retinas accumulate two carotenoids, lutein and zeaxanthin, as the **macular** pigment, which is most dense at the center of the fovea and declines rapidly in more peripheral regions. The retina also distributes alpha-tocopherol (vitamin E) in a nonuniform spatial pattern. The region of monkey retinas where carotenoids and vitamin E are both low corresponds with a locus where early signs of AMD often appear in humans. The combination of evidence suggests that carotenoids and antioxidant vitamins may help to retard some of the destructive processes in the retina and the retinal pigment epithelium that lead to age-related **degeneration** of the macula. Three patients with age-related **macular** **degeneration** for whom cataract surgery was indicated received low-power intraocular lenses (IOLs) calculated to produce an end spectacle refraction of approximately +6 diopters, producing a magnification of about 12%. Our experience with these three cases suggests that use of low-power **implants** in such patients may yield better results than emmetropic IOLs. AIM OF THE STUDY: The aim of this study is to test the effect of low dose radiation on the subfoveal neovascular membranes (SNVM) and to analyse visual acuity in age-related **macular** **degeneration.** METHODS AND PATIENTS: From November 1993 through to August 1994, 10 patients, on the one hand, were given a dose of 5 Gy followed by controls 6 weeks and 6 months later. On the other hand, 21 patients were treated with a dose of 8 Gy and were subjected to controls 6 weeks later. Before the radiotherapy and during the control sessions, all patients were required to be measured for different parameters of visual acuity and to receive a simultaneous fluorescein and indocyanine green angiography. The radiotherapy was done by a linear accelerator 6 MeV and through a lateral port 3 x 4 cm in half beam technic. RESULTS: In the 5 Gy group, no changes in the parameters for visual acuity were noted in most cases after 6 months. In 9 of the cases, the membranes had increased in size and in 1 case, they had remained unchanged. In the 8 Gy group, no changes in the visual acuity or in the membrane size were diagnosed. Of all the patients treated, only one refused the angiography control. DISCUSSION AND CONCLUSIONS: Given the low dose used and the period of observation, the visual acuity of all patients remained stable. The size of the membranes increased in most cases for those 5 Gy patients and in this respect, no changes at all were noted in the 8 Gy patients. In order to better evaluate the potential of radiotherapy, this study must be pursued and coupled with further studies analysing the effect of different doses on patients. AIM–To evaluate whether perifoveal **laser** photocoagulation of soft drusen reduces the total area occupied by drusen. METHOD–In a prospective, randomised study, 20 patients (mean age 71.3 (SD 7.7) years) with early age-related maculopathy (ARM) in the form of soft drusen and pigmentary changes and with good visual acuity (0.94 (0.09)) were treated with argon green **laser** photocoagulation. Mild **laser** burns (200 microns) were placed within a temporal horseshoe-shaped area, extending from a distance of no less than 500 microns from the centre of the fovea to the vascular arcades. They were placed on the drusen and scattered over areas where no drusen were present. Fundus colour photography and fluorescein angiography were performed at study entry as well as after 3 and 6 months. Nineteen age-matched patients (68.5 (6.2) years) with soft drusen maculopathy (visual acuity 0.95 (0.10)) were followed as a control group. Using a computer system, the area occupied by drusen was determined as a portion of the total area of a circle with a radius corresponding to 1250 microns in the fundus for the angiograms and 2500 microns for the colour photographs, respectively. At study entry, the mean area occupied by drusen in the **treatment** group was not significantly (p > 0.5-0.7) different from that of the control group. RESULTS–The mean drusen area of the angiograms and fundus colour photographs in the treated group decreased significantly from 19.3% to 13.8% (p = 0.002) and from 7.84% to 5.02% (p = 0.005), respectively. In the untreated group, the mean area occupied by drusen increased significantly from 17.4% to 20.4% (p = 0.030) and from 8.33% to 9.23% (p = 0.002), respectively. No significant changes in visual acuity (p > 0.05-0.5) or in visual fields (p > 0.05-0.3) occurred in either of the two groups during 6 months. CONCLUSION–The study suggests that the area occupied by soft drusen in patients with early ARM decreases after perifoveal **laser** photocoagulation but increases in an untreated control group. Since 1991 we have been gaining experience in the surgical removal of submacular subretinal membranes in patients with presumed ocular histoplasmosis syndrome (POHS), idiopathic subretinal neovascularisation, myopia and age-related **macular** **degeneration** (AMD). Seventeen patients were operated between 1991 and 1993. Significant improvement of vision was achieved in 4 out of 5 patients with POHS, 3 out of 5 with idiopathic neovascularisation, 2 out of 4 with myopia but none of 3 patients with AMD. The results suggest that subretinal neovascularisation can be successfully removed in POHS and in some forms of idiopathic neovascularisation and myopia but probably not in AMD. Dysfunction as well as pathological changes of retinal pigment epithelium (RPE) has been implicated as the causes of some retinal diseases, including age-related **macular** **degeneration,** hereditary **macular** **degeneration** and retinitis pigmentosa, etc. Transplantation of normal healthy RPE cells with an attempt to treat the retinal diseases is one of the current interests in ophthalmic research. We have developed a modified pars plana technique including vitrectomy for subretinal transplantation of homologous, cultured, natural pigment labelled RPE cells in the non-pigmented rabbit. Our results, with follow-up from one week to one year, revealed that the transplanted RPE cells not only survived and attached to Bruch’s membrane of the host eyes, but also had a distinct basal and apical morphology as seen in close contact with host photoreceptors, and formed junctional complexes with neighboring RPE cells. Close contact between the microvilli of the grafted RPE cells and the photoreceptor outer segments of the host was also observed. The normal periodical sheddings of the host outer segments were phagocytosed by the transplanted RPE cells, as demonstrated in our results. Furthermore, there was practically no, if any, sign of rejection found. All the results have demonstrated that the transplantation of RPE cells in rabbits was successful and these observations provide a reliable experimental evidence for the clinical research of allotransplantation of RPE cells. Non-neovascular AMD is usually not treated; instead patients are followed for the possible development of neovascular AMD. Although vitamin and mineral supplements have been sug,ested as a wav to slow the progression of non-neovascular AMD, there is no solid evidence to support this hypothesis. A major research study, sponsored bv the National Eye Institute of the National Institutes of Health, is currently testinc, whether vitamin and mineral supplements delay the progression of AMD. Results of the trial, called the Age-Related Eye Disease Study (AREDS), are not expected for more than five years The treatment of neovascular AMD is coagulation of new blood vessels with a laser. Because of its difficulty, photocoa-,ulation (as the laser treatment is called) for AMD must be carried out by an ophthalmologist with special training and experience. Such treatment has not proven to be useful in patients with poorly demarcated new vessels. Photocoagulation has, however, been shown to decrease the risk of visual loss in well-demarcated new vessels identified in extrafoveal, juxtafoveal, or subfoveal sites, according to the Macular Photocoagulation Studv. In patients with extrafoveal AMD in this study, severe visual loss occurred after 18 months in 60% of untreated eyes but in only 25% of treated eyes. Although benefits persisted for five years after treatment, they diminished over time. The recurrence rate after successful photocoagulation was 10% at one to two months, 24% after six months, and 54% after three years. A diminished risk of severe visual loss was also shown after photocoagulation of juxtafoveal and subfoveal vessels. The high incidence of recurrence of AMD necessitates careful followup and periodic fluorescein anglographv. Immediate re-examination is required for the onset of new symptoms of visual loss or distortion noted with self-monitoring using an Amsler grid. A close watch must be maintained on the other eye as well. For patients whose pattern of new vessels is not amenable to laser treatment, medical therapy with interferon, a drug that may cause the vessels to shrink, and a sur,ical procedure to excise the abnormal vessels (called subfoveal surgery) are being tested. Some studies indicate that certain factors within an individual’s control might play a role in the development of AMD. Avoiding excessive Possible Cause Found for Proliferative Retinopathy In a recent study, researchers detected a substance in eye fluid that may be at least one of the culprits responsible for the development of proliferative diabetic retinopathy (see pa-e 32). They sug- t, ,-est that the substance, vascular e ndothelial growth factor (VEGF), is secreted by cells in the lining of blood vessels (endothelium) in the eye in response to dama@e done to the blood vessels by diabetes, and that VEGF promotes the abnormal arowth of blood vessels characteristic of proliferative retinopathv. Researchers obtained samples of eye fluid from 164 patients who underwent eve sur-erv, either for diabetic retinopathv or for other conditions that do not involve new blood vessel @rowth in the eve, such as cataracts. VEGF was detected in 51′!’O of the patients with retinopathy, but in only 7% of those with other eve diseases. Moreover, the concentration of VEGF was nearly four times higher in the patients with active proliferative retinopathy than in those who had nonproliferative retinopathv or other eve diseases. Laser photocoagulation resulted in a 75% decline in VEGF levels in patients who underwent the procedure to treat proliferative retinopathv. Better understanding of the exact role VEGF plays in proliferative retinopathv could lead to improved screening tests and treatments. THE NEW ENGLAND JOURNAL OF MEDICINE VOLUME 331. NUMBER 22 December 1, 1994 1 9 9 5 n V I S I 0 N D I S 0 R D E R S exposure to sunlight was found to be protective in one large study. Men and women who spent more than three-quarters of their time outdoors in the summer were more than twice as likely to develop neovascular AMD than those who spent less than one-quarter of their time outside. Men who re@ularly wore sunglasses and a hat with a brim, however, reduced their risk of developing AMD bv 40%. Other studies have suggested that eating fruits and vegetables high in ‘ds, especially beta carotene, might help prevent AMD. In one carotenot I such study, patients with medium to high blood levels of carotenolds had one-half to onc-third the risk of developing AMD compared to those with the lowest levels. Carotenolds are yellow-orange pigments found in vellow, Oran-e, red, and dark rcen fruits and vegetables. Their potential protective effect is due to their antioxidant properties. Antioxidants help prevent cell dama-e within the body. More study is needed before definite recommendations can be made from these findings. Still, it is probably worthwhile to take steps to protect the eyes from UV ravs and to eat plenty of fr-ults and vegetables rich in carotenol ‘ds. Low-Vision Aids The needs of most people with vision loss are being unmet. Most commonly “Nothing more can be done” is told. Studies suggest that the average person with impaired vision has up to a 3 year delay for care. The leading forms of therapy are in identifying the causes of deterioration and preventing further damage and treating damage early if it occurs. The treatment centers on prevention and early detection. A disorder characterized by central vision loss with two main forms, wet and dry. The wet form results in hemorhage and loss of vision with metamorphopsia. The dry form is a slowly progressive damage. The key to treatment is: catch it early, Hereditary component warn family members vitamins, betacarotene, zinc, C, Ocuvite. Laser surgery often helpful for sudden changes. AMD leads to low vision in some affected individuals. The loss of vision is often accompanied by depression, loss of self-image, grief, and even ‘ ‘de. A number of low-v’s’on opt’cal a’ds can be ut’l’zed to opt’m’ suici 1 1 i ize remaining vision. The perceived benefits of these aids, most readily ‘lable at a low-vision rehab’l’tat’on center, depend on the expecta- aval 11 I tions of the patient. Those with unrealistic expectations are likely to be disappointed, while many with more realistic expectations will recog’ ‘f’cant benefits. These a’ds ‘nclude: nize signi 1 1 1 0 For close work, a pair of high-power reading glasses (available at the local drug storc) or a large magnifying glass with a built-in light. A variety of high-power loupes (which are clipped onto the glasses) and magni 1 ‘f’ers (hand-held, w’th stands, or with lights) can be prescribed by an ophthalmoloc,ist. For intermediate and distance vision, a variety of hand-held, clip-on, and spectacle-mounted telescopes are available. A small telescope can be mounted on one lens of a pair of glasses so that it can swin, into use Z:) for watching television. Since this type of telescope would be cumbersome and confusing for walking around, a pocket telescope may also be needed. – A closed-circuit television hookup, though expensive, can provide up to 60x magnification. This device works by displaying ob’ects put in front of a camera onto a television screen. It can make reading, wnting, and 1 ible for those w’th severe v’s’on loss. typ ng poss 1 1 1 o A new system, the Low Vision Enhancement System (LVES) has been developed by collaborators at Johns Hopkins, NASA, and the Veterans Low Vision Services/Aids With magnifying glasses and new telescopic devices images can be enlarged many fold. Therer are close circuit TV’s to magnify images, scanners with computers and devices that hook up to any TV. All these devices are technologically advanced and quite expensive, but for many, well worth it. Low Vision Services/Aids With magnifying glasses and new telescopic devices images can be enlarged many fold. Therer are close circuit TV’s to magnify images, scanners with computers and devices that hook up to any TV. All these devices are technologically advanced and quite expensive, but for many, well worth it. Evansville Association for the Blind 30 Lowering Retinopathy Risk Carefully monitoring and adjl blood glucose levels reduces th of diabetic retinopathy, accordt more detailed results from the betes Control and Complic@, Trial of over 1,400 subjects, age 39, with insulin-dependent di@ mellitus (IDDM). The triai di, include patients with non-in. dependent diabetes (NIDDM), i is more common, but the r should hold true for them as we Subjects were divided intc, ,aroup of patients who had IDD one to five years and had no si@retinopathy, and another IDDM for one to 15 years and mal to moderate nonprolifer retinopathy. Patients received e intensive or conventional thei Intensive therapy consisted of i or four insulin (a hormone usk control blood sugar levels) sh( day or continuous insulin infus along with blood glucose tests or four times daily. Convent therapy was one or two insulin I tions a day. Retinal photogr were used to detect retinopathv. In the group starting with n tinopathy, intensive therapy lo@, the risk of developing retinor over nine years by 27%, compai conventional therapy. Subjects some signs of retinopathy who intensive control had a 34% tc lower risk of pro-ression than on conventional therapy. The s the risk reduction depended on intensive treatment was starte, the extent of initial retinopath the study’s authors conclude, “I sive therapv should form the bone of any healthcare str aimed at reducing the risk of loss from diabetic retinopathy.” OPHTHALMOLOGY VOLUME 102, NUMBER 4 .4pril 1995 Administration. The LVES is a pair of tiny head mounted television screens and cameras that project ‘mages directly ‘n front of the eyes. – Large-print books and newspapers are available, as are a wide variety of household products with lar@e images, such as clocks, telephones, Z:) playing cards, address books, calculators, cassette players, sewing accessories, and writing supplies. End Stage Glaucoma. Glaucoma creates a loss of peripheral (side) vision. Left uncontrolled patients go blind, in fact thousands do yearly. Control is critical with glaucoma surgery. New developments are Setons, and new medications prostaglandins or hormones, and blood pressure medications. Retinal Detachments. Caught early the success is >80% The retina peels off the wall of the eye resulting in the loss of vision much as a curtain would do. Clear Cornea Catarct Surgery This technique spares blood vessels and eliminates unnessary steps. Patients recover more quickly and can be in new glasses as early as one week. End Stage Glaucoma. Glaucoma creates a loss of peripheral (side) vision. Left uncontrolled patients go blind, in fact thousands do yearly. Control is critical with glaucoma surgery. New developments are Setons, and new medications prostaglandins or hormones, and blood pressure medications. Retinal Detachments. Caught early the success is >80% The retina peels off the wall of the eye resulting in the loss of vision much as a curtain would do. Clear Cornea Catarct Surgery This technique spares blood vessels and eliminates unnessary steps. Patients recover more quickly and can be in new glasses as early as one week. Second Opinions Often one is told that nothing else can be done. Never hurts to seek another opinion.